Saving Lives Through a Daring Medical Breakthrough

1. Introduction
Boston Children’s Hospital’s pioneering use of mitochondrial transplantation in clinical settings offers the potential to transform not only open heart surgery but modern medicine as a whole. We are proud to have funded the technology that first turned this promising new approach into a practical reality and helped save the precious lives of infants and children.
Introduction
In 2014, a mother named Jessica Blais got the devastating news from doctors at Boston Children’s Hospital (BCH) that her infant daughter, Avery Gagnon, suffered from a potentially fatal heart defect and would need surgery.
“They performed heart surgery,” Jessica recalls. “Everything was fine. But her heart wasn’t working right again. It was very scary, and I thought I’d be burying my daughter by Mother’s Day.”
Avery’s dire condition necessitated using a daring and pioneering treatment. Led by Dr. Jim McCully, a team of doctors and researchers at BCH—one of the world’s leaders in pediatric research and the main pediatric program of Harvard Medical School—were determined to do just that. This new, experimental technique, which they had only recently devised, was called mitochondrial transplantation.
If successful, the trial would prove the technique’s safety in humans and drive progress in advancing new treatment options for infants with heart issues and patients with other diseases.
“That was emotional because it was an early one,” Dr. McCully recalls today. “[Avery] was a particularly challenging case. It’s always a really big deal for everyone, you know, any time you’re working on a child, it’s a big deal.”

A Revolutionary Approach: Mitochondrial Transplantation
A few months earlier, Dr. McCully had come to BCH convinced that the use of mitochondria might have significant therapeutic value—especially for children, like Avery, with health problems so severe they might not survive infancy. Mitochondria are commonly referred to as “the powerhouses of the cell,” because they generate the molecule ATP, adenosine triphosphate, which stores the energy from a human’s food intake and allows it to fuel many of the cell’s other components.
When the mitochondria are malfunctioning, as happens with a serious cardiac problem, no external drug treatments can repair damage to the tiny oval cellular structures, which can leak or swell, depriving the cell of the energy it needs to allow the heart to beat regularly and the heart tissue to rebuild.
“I had thought that perhaps there was another option,” notes McCully. He had developed a promising technique, funded by the National Institutes of Health, that isolated healthy mitochondria and transplanted them into the damaged tissue of live mice and pigs.
Invited to Boston Children’s Hospital by Dr. Pedro del Nido, chairman of the department of Cardiac Surgery, to expand his research, McCully and his colleagues had a breakthrough idea: the mitochondria of an ailing infant might be extracted during an operation, harvested, and reinjected into the same patient’s heart to restore its functioning.
“It definitely was an a-ha! moment for Jim, because a litany of therapies had been tested to recover mitochondria in the body... and a lot of things looked promising in the lab, but when they went to the clinic, there was no result—until Jim said: 'well, why don't we just take healthy mitochondria and inject them?' ”
“It was quite controversial, risky, courageous, foolish—call it what you will,” observes Dr. Sitaram Emani, a BCH surgeon and a colleague of Dr. McCully and Dr. del Nido’s. “But we had no other choice. I mean, we knew that these patients would die without any additional help.”
Doctors utilized the technique on an initial group of infants with serious cardiac conditions, all of whom would otherwise likely die without a medical intervention. In Avery Gagnon’s case, she survived. The transplantation procedure meaningfully improved her heart function, enabling her to be removed from a life-support machine and move toward a full recovery.
The positive results of the procedure were obvious and amazingly swift. “When you inject the mitochondria, the heart changes.” McCully observes. “When it’s not beating, it’s sort of very grayish and ugly looking, and it just sits there. When you put the mitochondria in, it comes back. It’s viable. It starts beating, and it’s pink. So it’s instant gratification for the surgeons. It comes back within our babies within about 10 to 15 minutes.”
Speeding the Process
Buoyed by this early success, McCully and his colleagues looked to turn mitochondrial transplantation into a standard procedure, widely used and adopted, with the potential to save hundreds or thousands of lives. But there was a daunting logistical problem: the technique called for the mitochondria to be removed while the patient was in open heart surgery, with their chest open and heart exposed. Removing a small sample from the patient’s abdominal muscle, McCully would carry it to a lab, process it through an elaborate biological procedure in another area, then return it to the operating room where Dr. Emani re-injected the harvested mitochondria directly in the heart. All while the infant remained fully anesthetized, with his or her heart stopped—a potentially dangerous situation.
To solve the problem, Dr. McCully and his colleagues came up with an ingenious concept: a portable, sterile “hood” that could carry out the mitochondrial harvesting right in the operating room, saving critical time and reducing risk. But the hundreds of thousands of dollars in funds commonly received from government agencies or sourced internally to develop this state-of-the-art device were out of the question. To bridge this “chasm,” in the words of Dr. Pedro del Nido, the hospital turned to Griffin Catalyst, whose $500,000 seed grant in 2016 allowed the first prototype to be built. “The hood itself is a table that’s on wheels,” McCully explains. “It has a vent, special air flow, special lights, special window, special wiring, and all of materials inside.”
We were able to develop a procedure that is now used throughout the world. It normally used to take two hours to isolate these mitochondria. This allows us to do this in 20 minutes. [With the new device] everything’s sterilized, and then we get a small piece of tissue, and then I do my procedure within 20 minutes, and we can hand them back purified mitochondria we’ve already checked, and it goes back in rapidly. So this device that Ken Griffin was able to give us allows us to be right beside the patient.
Growth Around the World
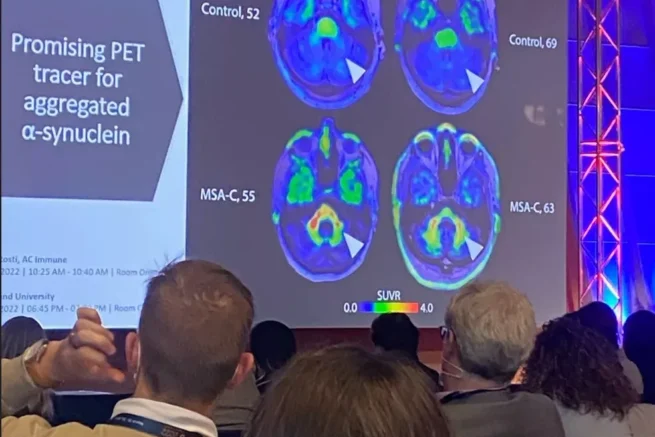
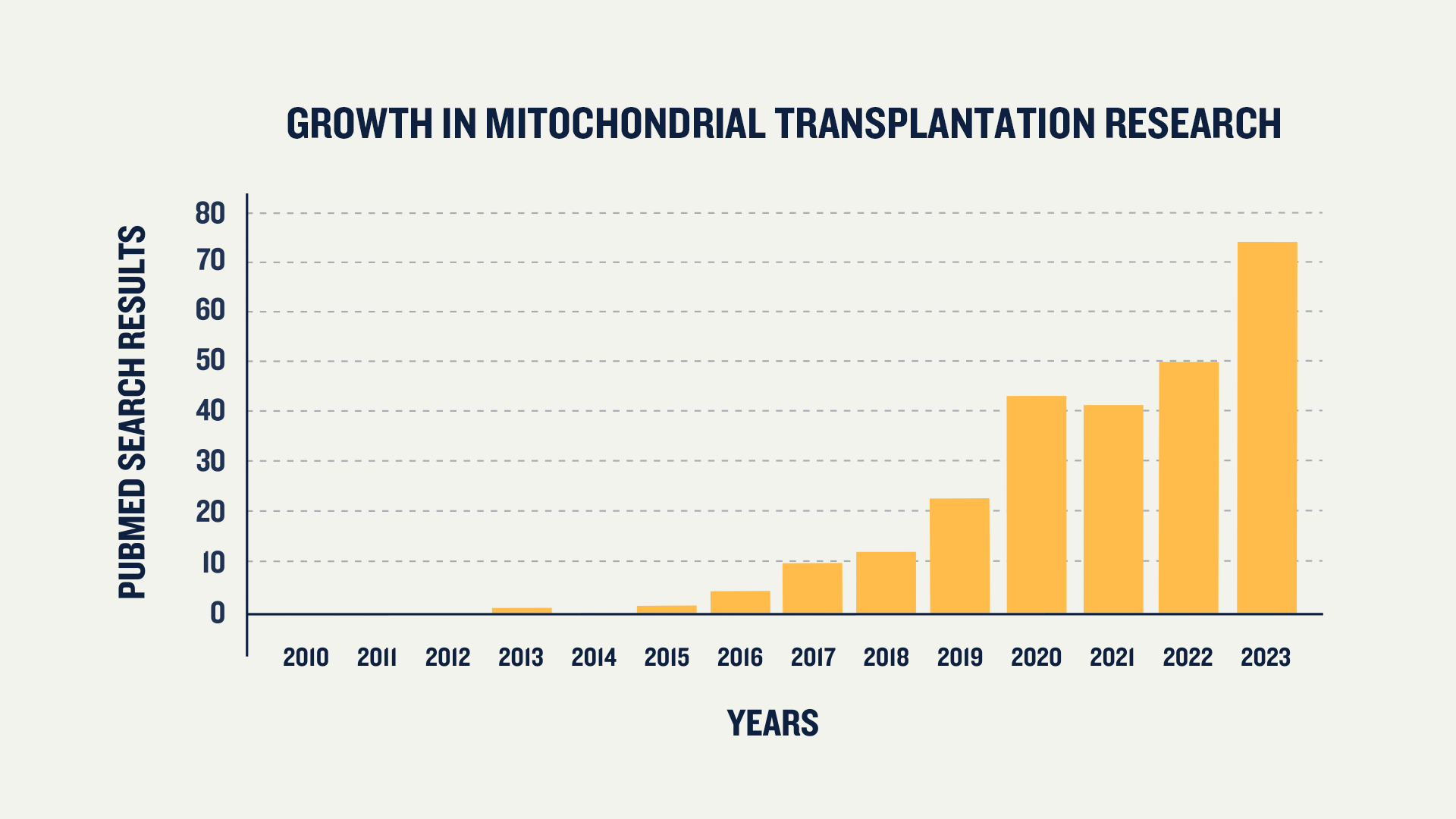
Since those early years, the potential therapeutic use of mitochondrial transplantation—and the vital piece of equipment that made it possible—has been extended through research around the globe, expanding its impact to countless human systems, including not only the heart but the brain, kidney, lung, muscle, and eyes. “It’s really revolutionary; 10 years [ago] there was nothing about it, and it’s now all over the world,” observes Jennifer Hagen, Associate Vice President at Boston Children’s Hospital Trust.
“It’s just exploding even in fields that we never even imagined. For example, cancer. We never even imagined that there would be a role for this. It wasn’t even on the radar screen. But there is evidence that it’ll work there. And it’s not just children, it’s adults. It’s everybody. So yeah, it’s been really quite amazing to watch.”
Thanks to this innovative technique—and the early funding from Griffin Catalyst that allowed it to become a reality—Avery Gagnon is today an active 9-year-old girl. “She’s done well,” McCully observes proudly. “She even went through her ‘terrible twos,’ according to her mother, Jessica. We still get Christmas cards from them.”
Today, Avery’s mother, Jessica, reports her daughter enjoys drawing, dress-up, and ballet and jazz dance classes.
“After she had the procedure eight years ago, when we almost lost her, I said, 'you know what? If we get through this, I want to know that if I ever lose her, I want to know that she lived.' And now, if she’s gone tomorrow, I want to be able to say, 'look at everything she did in these eight years we had her.' I want her to spread her wings and—within reason and obviously within safety—I want to know that she lived and she got to adventure and got to do all these things [with her life].”